
Combined medical research training shines light on mosaicism, implications in genetic mutations
Imagine you have a child with a severe genetic disorder. You love him dearly, but caring for him takes every waking moment and has strained the relationship with your partner. Despite these challenges, you’ve decided you want to have another child. You visit your geneticist, and she explains that because your child’s disease is caused by a new DNA mutation, not found in either you or your partner, a recurrence is extremely unlikely—less than 1 percent.
A little more than a year later, you take your beautiful new baby home. But, after a few months, you notice that he is beginning to seem more and more like his brother. A genetic test confirms your worst fears; your new second born has the same mutation.
How could this happen? What could have been done differently?
When applying to M.D./Ph.D. programs, interviewers always ask, “Why do you want to pursue a dual degree?” The answer I gave then and I still believe now is that combined medical and research training helps identify and tackle the questions that have a tangible impact on human health.
Early in my genetics training at Baylor College of Medicine, I had the opportunity to meet an adorable young girl at Texas Children’s Hospital. She was being assessed because genetic testing found a mutation that had never been reported. As part of a research study into her condition, I discovered that her father also had a few cells in his blood with the same mutation. This surprised us because he seemed completely healthy. Careful examination found the mutation in 1-2 percent of his blood cells, a level so low that it was missed by clinical tests.
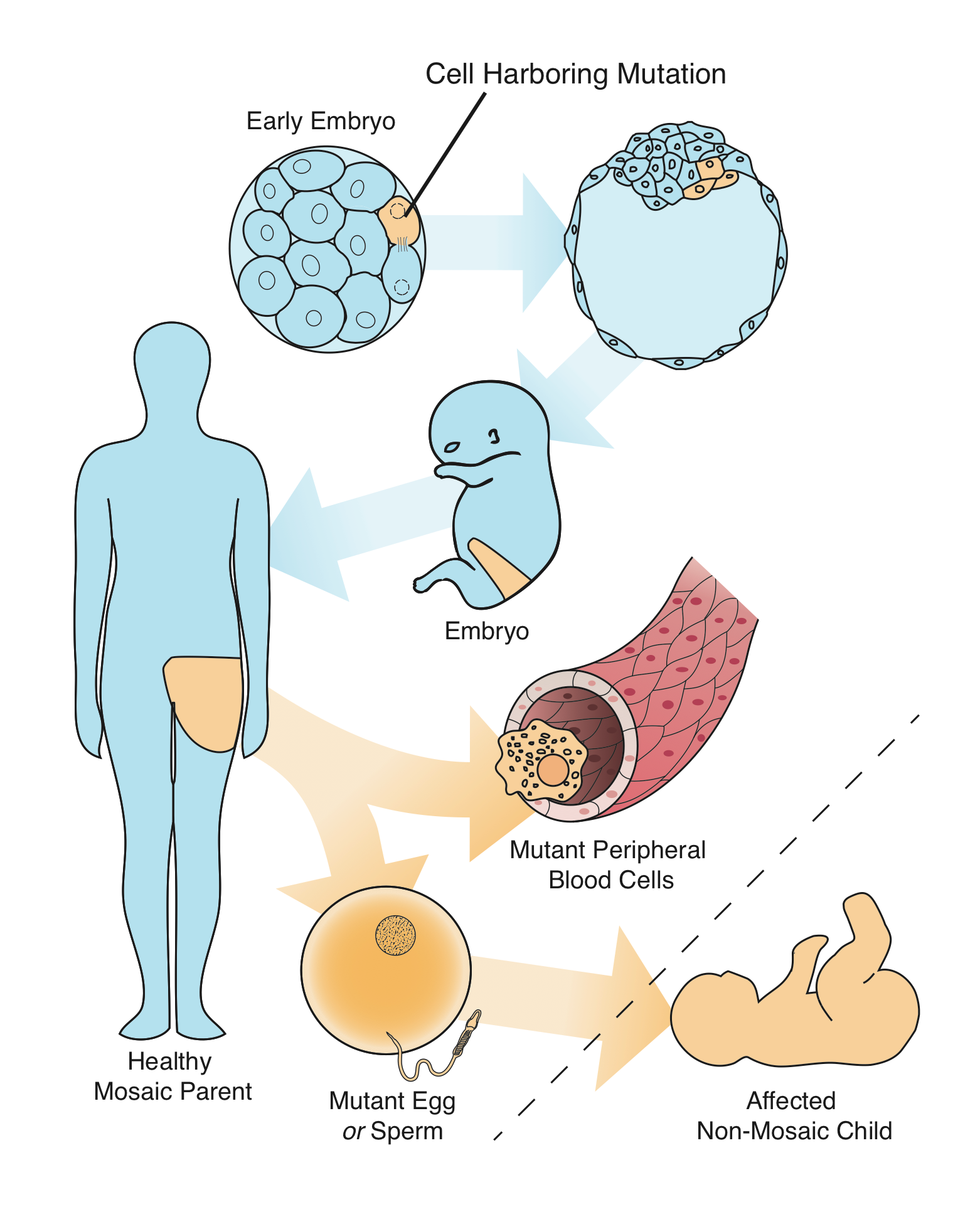
Our data suggested that the father is mosaic for the mutation found in his daughter. Mosaicism is defined as the presence of two or more populations of cells within the same organism with different genetic makeup. The mutation actually occurred in the father sometime during his development. The mutant cells then made their way into both his blood cells and his sperm.
Cutting-edge genetic research suggests mosaicism happens in all of us and is associated with aging and cancer. However, mosaicism has also been found in families with unexpected recurrence of genetic disease. The father in our study was expectedly worried about what mosaicism may mean for his risk of having a second, affected child. This was especially important because he and his wife were planning to have another child. Unfortunately, our lack of knowledge made our guidance less than satisfying.
My thesis mentors, Drs. Jim Lupski and Paweł Stankiewicz, and I wondered if mosaicism in parents for mutations found in their children might be more common than appreciated. Likewise, we hoped studying the issue could help us understand how mosaicism influences recurrence risk.
I applied for and received a fellowship from the NIH National Institute for Neurological Disease and Stroke to fund the study and set about the long process of obtaining DNA samples to answer our questions. We recruited families not only from here in Houston but also from our friends and collaborators in Belgium, the Netherlands, Poland, and the United Kingdom. After three years, we had finally collected and tested 100 families for mosaicism. We found four cases where a parent was mosaic, a rate higher than even we expected.
With our observations as a basis, we also developed a probabilistic model of development and fertilization to answer our second question, what does mosaicism mean for parents? We enlisted the help of Dr. Chad Shaw, an associate professor at Baylor with an adjunct appointment in Statistics at Rice University. Our model suggests that mosaicism increases a parent’s risk of recurrence by more than an order of magnitude. In some cases, the risk could be much higher than the quoted “less than 1 percent,” even 5 percent or more. See mathematical model.
Our study was published July 31 in the American Journal of Human Genetics. It’s an exciting experience that brings a sense of relief when years or work finally reaches a conclusion. Likewise, seeing it reported in the New York Times gives the time and effort spent by so many people across the globe an extra sense of meaning.
Although additional research will be needed, our results lay the foundation for sensitive tests for mosaicism that may help geneticists improve recurrence risk counseling for couples with a child with genetic disease.
If you found yourself in such a situation, would you spend the time and expense to better understand your risk? Let us know in the comments below.
–By Ian Campbell


Mosaicism is one of the most complicated issues in genetics. We have a long way to go. Yes, I will spend time on it